

FINDING THE DATA ON MISSING GIRLS
Context:
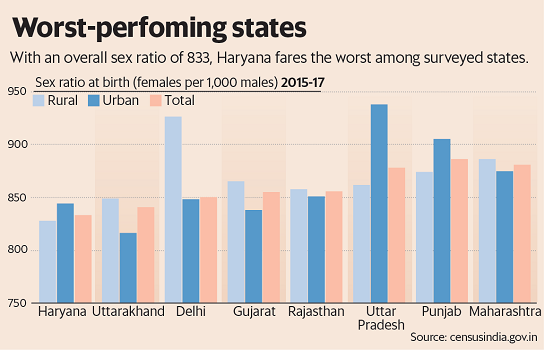
- The recently released Sample Registration System (SRS) data for the period 2015-2017, shows the drastic fall in Sex Ratio at Birth (SRB) Rate and the rapid increase in the female foeticide all over the country.
Introduction:
- India has one of the highest female foeticide incidents in the world.
- The female child population in the age group of 0-6 years declined from 78.83 million in 2001 to 75.84 million in 2011.
- During the period 1991-2011, the child sex ratio (0-6 years) declined from 945 to 914.
- The sex ratio at birth (SRB) has been dropping continuously since Census 2011, coming down from 909 girls per thousand boys in 2011-2013 to 896 girls in 2015-2017, to quote the yearly SRS Statistical Reports.
- In the 2014-2016 period, of the 21 large States, only two — Kerala and Chhattisgarh had an SRB of above 950 girls per 1000 boys.
- Thus, at present, about 5% of girls are ‘eliminated’ before they are born, despite the promises of the Beti Bachao Beti Padhao scheme.
What Is Health Management Information System (HMIS)?
- HMIS is an online portal that provides information on health indicators in India.
- HMIS compiles data from state- and district-level health authorities, the National Family Health Survey (NFHS), the District Level Household Survey (DLHS), and the Office of the Registrar General & Census Commissioner, among other sources.
- It is a fundamentally awed source that largely considers home deliveries and births in government institutions.
- Data from the HMIS are incomplete and not representative of the country as a whole as births happening in private institutions are under-reported.
- The HMIS report itself acknowledges that based on the estimated number of births, the number of reported births is much less in both the years considered — 2015-16 and 2018-19.
- Thus, private hospitals had a disproportionate excess of male children births, which the HMIS sample excludes.
Health Management Information System (HMIS):
- Health Management Information System (HMIS), a fundamentally awed source that largely considers home deliveries and births in government institutions.
- Data from the HMIS are incomplete and not representative of the country as a whole as births happening in private institutions are under-reported.
- The HMIS report itself acknowledges that based on the estimated number of births, the number of reported births is much less in both the years considered — 2015-16 and 2018-19.
Difference among points of Delivery:
- The differences among the three points of delivery become evident when SRB is calculated using data from National Family Health Survey-4 (NFHS-4).
- Of the 2.5 lakh reported births in the 2010-2014 period, the distribution of births at home, government hospitals and private hospitals was 21%, 52% and 27% respectively and the corresponding SRB figures were 969, 930 and 851.
Reasons for use of NFHS Data:
- Data for the private sector are more skewed and it has not been articulated in the NFHS reports or adequately dealt with by the Health Ministry.
- For two decades, in visits to hospitals, particularly private, too often we observed more male children even when the total number of births were small in number. So, we used NFHS 4 data to quantify this bias.
- It is criminal to use public funds to privilege boy births and facilitate discrimination against girls right from birth. However, for years, in the special neonatal care units (SNCU) set up by the government, there was an excess of about 8% male children in several States.
BIAS over First-Born child:
- Our field visits to various parts of India in the past five years, particularly in Uttar Pradesh and Bihar, where one in every three Indians is born, revealed a massive expansion of ultrasound clinics even in remote corners.
- And in the absence of a stringent implementation of the Pre-Conception and Pre-Natal Diagnostic Techniques (Prohibition of Sex Selection) Act (PCPNDT Act), practically anyone who wants to determine the sex of the foetus is able to get it done illegally.
- Therefore, the increased deterrence in States like Maharashtra, Haryana and Rajasthan in recent years has been undermined by the laxity of the biggest States.
- The Indian Medical Association (IMA) has to ensure that private hospitals don’t profit from discrimination against girls before birth.
Gender BIAS:
- For two decades, private hospitals had more male children even when the total number of births were small in number. So, NFHS 4(National Family Health Survey 4) data was used to quantify this bias.
Reasons for this BIAS:
- In the special neonatal care units (SNCU) set up by the government, there was an excess of about 8% of male children in several States for years.
- Bias occurs when the firstborn child comes into the picture— the SRB among firstborn children was 927, meaning that 2.5% of firstborn girls are eliminated before birth.
- A massive expansion of ultrasound clinics even in remote corners especially of Uttar Pradesh and Bihar.
- Anyone who wants to determine the sex of the fetus was able to get it done illegally due to the absence of stringent implementation of the Preconception and Prenatal Diagnostic Techniques (Prohibition of Sex Selection) Act (PCPNDT Act)
- Central Supervisory Board established under the PCPNDT Act has not met for over one and a half years.
- Regrettably, the government has prioritized an expansion of SNCUs rather than deal with the issue of the ‘missing girls’. Protecting the integrity of birth statistics will help the people, governments and health professionals to focus on ameliorating the known gender gaps at birth rather than be complacent with dubious claims.
Initiatives Taken by The Government:
- Apart from Pre-conception and Pre-natal Diagnostic Techniques (Regulation and Prevention of Misuse) Act, 1994 (PCPNDT Act) to address the issue of sex-selective abortion, India also enacted the Medical Termination of Pregnancy (MTP) Act in 1971 to regulate access to safe abortions.
- The MTP Act of 1971, amended in 2002, allows abortion up to 20 weeks of pregnancy in cases where “the continuance of the pregnancy would involve a risk to the life of the pregnant woman or of grave injury to her physical or mental health”.
- The Ministry of Health and Family Welfare has acknowledged that illegal abortions still outnumber legal abortions and thousands of women die every year due to complications resulting from unsafe abortions.
- The under-reporting under the MTP Act has also been a problem.
- Schemes by Govt. of India: In a bid to encourage families to have girl children, prevent female foeticide and educate the girl child, the government launched:
- Beti Bachao, Beti Padhao campaign in January 2015.
- Conditional cash transfer schemes such as Balika Samriddhi Yojana and Dhanalakshmi Scheme.
Way Ahead:
- Medical associations should fulfill their obligation to follow the law.
- The Indian Medical Association (IMA) has to ensure that private hospitals don’t profit from
- discrimination against girls before birth.
- Health Minister restores the regularity of the meetings of Central Supervisory Board established under the PCPNDT Act.
- Implementation of the Preconception and Prenatal Diagnostic Techniques (Prohibition of Sex Selection) Act (PCPNDT Act) should be done in such a way that no one can determine the sex of the foetus.
- Protecting the integrity of birth statistics will help the people, governments and health
- professionals to focus on improving the known gender gaps at birth rather than be self-satisfied with dubious claims.
Source: The Hindu



